
Schedule a
Menstrual Bleeding Treatment Consultation
Please call 508-947-0800 or fill out the form below
By submitting this form you agree to be contacted via phone/email
Menstrual Bleeding: What Is Abnormal Bleeding and What Does It Mean
For most women, menstruation is a significant aspect of their child-bearing years. However, periods affect women differently. Characteristics , like how long a period lasts, how often a women gets her period, and how heavy her flow is, can differ from one woman to the next. Some of these differences are normal. However, some of them are not and may warrant further examination.
Abnormal bleeding, which may include heavy bleeding, bleeding too often, bleeding in between periods, or certain deviations from your normal menstrual patterns, can be a message that something is not right. It is important not to ignore abnormal bleeding, even if abnormal bleeding is normal for you.
Continue reading to learn more about abnormal bleeding. You’ll learn about the signs and symptoms to watch out for regarding menstruation, how to understand and record your menstrual patterns, find out if the features of your period are normal or abnormal, determine if your situation warrants a visit to your doctor, what tests and treatments your doctor can offer, and what underlying causes may be behind your abnormal bleeding.
Meet Dr. Edelman
Learn more about abnormal bleeding from Julia Edelman, M.D., F.A.C.O.G. NCMP. Dr. Edelman is a board certified gynecologist and a certified menopause clinician. Her expertise in the field of women’s health includes her residency at Brigham and Women’s Hospital in Boston and teaching medicine at Harvard Medical School as well as publications for medical colleagues and her book Menopause Matters: Your Guide to a Long and Healthy Life.
At Women’s Health and Gynecology of New England, PC, a private practice in Southeastern Massachusetts, Dr. Edelman provides her patients with resources and state-of-the-art treatments and technologies that help them with abnormal, heavy, prolonged, or any other type of irregular bleeding.
BASIC ANATOMY OF A PERIOD
MENSTRUATION AND AGE
It’s estimated that up to 35% of women experience heavy or prolonged bleeding (menorrhagia or abnormal uterine bleeding). However, abnormal bleeding is often unrecognized by women. For those who do notice abnormalities, many never report their symptoms. Therefore, the percentage of women may be much higher.
- BEFORE 35
Abnormal or prolonged bleeding is most common when a girl first begins to menstruate (menarche).
- AFTER 35
- PERIMENOPAUSE
Abnormal bleeding is a common symptom of perimenopause (the period right before menopause.) In fact, irregular bleeding patterns is the most common symptom of perimenopause. 8 out of 10 women will experience changes in their menstrual cycle when they enter this period.
While abnormal uterine bleeding is usually caused by hormone imbalances, it may be a sign of something more serious. Especially for women in perimenopause. For women over age 35, it is more common for abnormal or prolonged bleeding to have underlying physical or structural causes, such as polyps or fibroids.
According to Dr. Edelman, “During perimenopause, your menstrual flow may become lighter or heavier. You may bleed for longer or shorter periods of time. You may miss periods or bleed more often.”
According to Dr. Edelman, “Your uterus sends messages in several ways. Abnormal uterine bleeding is one of them. “
Types of Menstrual Bleeding
It is important to know how to differentiate between normal bleeding and abnormal bleeding.
NORMAL BLEEDING (YOUR MENSTRUAL PATTERN)
Every woman menstruates differently. It’s important to know your own patterns. This often requires keeping track of your period.
ABNORMAL BLEEDING
Abnormal uterine bleeding is when you:
- bleed (or spot) in between your monthly periods
- have extremely heavy periods
- Have prolonged periods
- Skip more than three menstrual periods in a row
However, “abnormal bleeding” may also refer to any deviation from your usual menstrual pattern.
Even though abnormal bleeding is common it is still abnormal. Abnormal bleeding is a prevalent problem, affecting more than 10 million women in the US.
ABNORMAL BLEEDING CAN TAKE MANY FORMS:
- Heavy bleeding:
- Or prolonged bleeding or prolonged and heavy bleeding (Menorrhagia)
- Large blood clots
- Bleeding too frequently
- Less than 21 DAYS from starting one menstrual period to starting next bleeding episode
- Prolonged Bleeding: (Bleeding for too long)
- More than 8 days or more than 3 days longer than your usual length menstrual period
- Spotting
- Spotting in between periods
- after menopause
- Irregular Menses: Skipping your period
- More than three months at a time?
- More than a year?
- Bleeding after sex
- Never normal
- Bleeding after menopause
- Bleeding after the final menstrual period is never normal even if it looks like a normal period
Maintaining a Menstruation History
The best way to recognize abnormal bleeding is establishing a baseline of your usual bleeding patterns.
Dr. Edelman encourages all her patients to keep track of their bleeding patterns. The more information you provide your doctor, the easier it will be to recognize any deviations from your normal patterns. “The key to identifying abnormal bleeding is keeping an accurate menstrual chart or calendar.”
Menstrual Calendar, App, or Chart
There are several ways to record of your menstrual history. Some women make note on their calendars. Other women make a dedicated chart or page in their journal. Some women download apps that record inputted data. The best method is whichever one works best for you.
WHAT TO KEEP RECORD OF:
When recording your menstrual cycle, keep track of the following:
The length of your menstrual cycle is calculated by the number of days between periods or “bleeding episodes.” The calculation starts on the first day of your period and goes to the first day of your next period.
When recording cycle length, it doesn’t matter when your period ends, just when it starts.
For example, if a woman started her period on June 1, bled for seven days, and then gets her next period on June 21, that would be a 21 day cycle. Whether she bleeds for 3 consecutive days or 7 days, her cycle length will still be 21 days.
The length of your menstrual period refers to how long your period lasts: from the day you start bleeding, to the day you stop.
Keep track of every day your bleed or spot during your period. Record any day(s) when you do not bleed while menstruating.
How many days do you have a heavy flow or see clots? How many days do you have spotting or light flow?
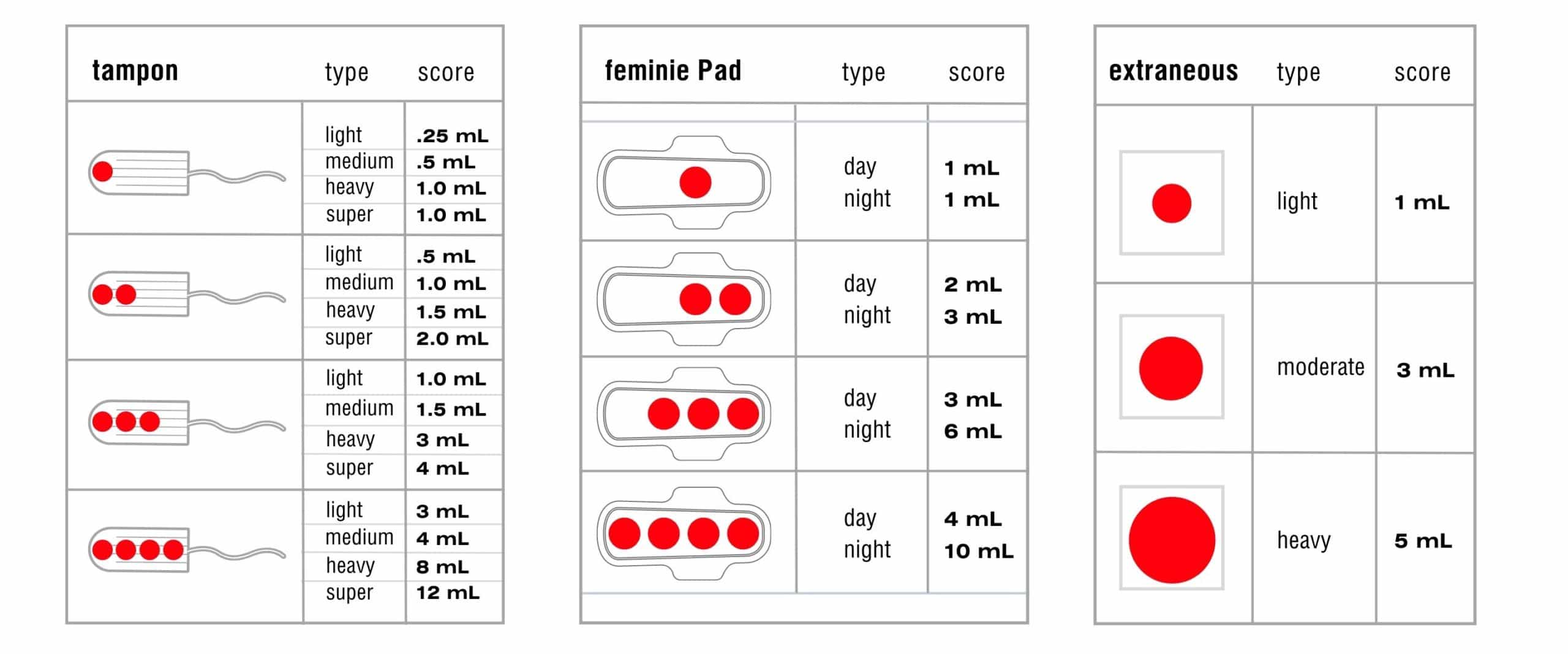
How much are you really bleeding? It is very difficult to judge how much blood you are losing during a menstrual period. You may think you know how much blood you lose during menstruation. But, blood loss can be deceiving. Studies show that a woman’s assessment on how much blood she is losing is seldom accurate.
One of the more reliable ways to measure the flow of your period is by counting the pads or tampons you go through. Also record the absorbency capacity of the feminine product you use. Is it a light maxi pad or a super absorbent tampon, etc.?
Large clots are often a sign of heavy bleeding.
If you notice clotting, record the size of the blood clot. Use coins as comparison. For example, was the blood clot the size of a dime? Or maybe it’s the size of a quarter.
Take note of any spotting in between periods.
Is Your Bleeding Abnormal?
There may be characteristics of your usual bleeding pattern that are in fact, not normal. Some features may be completely fine. Others warrant an assessment by your gynecologist.
Take the quiz:
What to Do if You Have Abnormal Bleeding
If you answered “yes” to any of these questions, you should seek a medical evaluation. Talk to your doctor or a find a reputable gynecologist in your area.
When seeing your doctor, make sure to bring the data from your menstrual chart, app, or journal. Knowing your bleeding patterns is very helpful for determining if your abnormal bleeding warrants further investigation.
Your doctor will consider medical history, menstrual history, age (stage of menopause) and possibly a pelvic examination to determine which course of action is best for you.
PROBLEMS:
- Thyroid Disease
- Sexually Transmitted Infection (STI)
- Polyps
- Fibroids
- Adenomyosis
- Endometrial Hyperplasia
- Uterine Cancer
- Endometriosis
- medications
- infection
- some forms of contraception
CAUSES OF ABNORMAL BLEEDING
Many things may cause abnormal vaginal bleeding. However, the two most common are hormonal imbalances that lead to ovulation disorders and structural abnormalities of the uterus. Structural or physical changes in the uterus are more common in women over 35 and women who are overweight or obese even if they are in their 20’s or early thirties.
Other causes include gynecological cancers, reproductive system infections, medications, retained foreign bodies, trauma, diseases, and other medical conditions.
HORMONAL CAUSES of IRREGULAR BLEEDING
Hormones play an integral part in the female reproductive system. Consequently, hormonal imbalances are the main cause of abnormal uterine bleeding. Hormonal imbalances that affect the menstrual cycle happen more often in younger women just starting their period and mid-life women transitioning through perimenopause.
Typically, hormonal imbalances that lead to abnormal bleeding are caused by an excess production of estrogen or the underproduction of progesterone.
Anovulation occurs when a woman does not ovulate during her menstrual cycle. During ovulation, the ovary releases an oocyte (egg) into the fallopian tube. If the egg is fertilized, the egg will attach to the endometrium (the wall of the uterus.) The endometrium thickens in preparation for pregnancy. However, if the egg is not fertilized, the body sheds the endometrium. This shedding is what causes bleeding during normal menstruation.
When an egg is not released during the menstrual cycle (anovulation), the body does not know to shed the endometrium (uterine lining.) This causes the lining to build up, becoming thicker and thicker, until it collapses, leading to heavy bleeding. This heavy bleeding looks like a menstrual period.
Anovulation has many causes. The most common, however, is hormonal imbalance.
Hormonal contraceptives are often used to control irregular or heavy bleeding, even in cases where contraception is not needed. At the same time there may be adjustment bleeding that takes place while the contraceptive begins to work. This may be true for many types of contraception including birth control pills, an injection with Depo-Provera ( a progesterone contraception), intrauterine devices (IUD’s), vaginal inserts (the NuvaRing or Annovera) and injectables (like Implanon).
Spotting in between periods and breakthrough bleeding (unexpected uterine bleeding that requires a tampon or sanitary pad) is the most common type of abnormal bleeding.
Hormone replacement therapy may be used to treat symptoms of menopause, such as hot flashes. Your doctor may offer bio-identical hormones to replace the hormones, like estrogen your body stops producing during menopause.
Hormone therapy may cause anything from light spotting to bleeding that mimics a normal period. If you experience bleeding after hormone replacement therapy, consult your gynecologist or doctor.
Abnormal uterine bleeding is a symptom of polycystic ovarian syndrome (PCOS). PCOS is often caused by a hormonal imbalance that results in anovulation (when your body does not release an egg during your menstrual cycle.) In this situation, too much estrogen causes the endometrium (the lining of the uterus) to thicken, while a lack of progesterone fails to signal the release of the endometrium.
Excess weight or changes in weight can cause irregular bleeding. Adipose tissue (fat) produces a weak estrogen, Estrone, that is different from the estrogen made in your ovaries. Too much adipose tissue may lead to an excess of estrogen. Estrogen may cause anovulation and lead to the buildup of the uterine lining. Recent research also suggests that excess weight may cause inflammation of the womb lining, causing delayed womb repair.
STRUCTURAL ABNORMALITIES
The second most common cause of irregular bleeding is lesions, also known as structural abnormalities, in and around the uterus. The most common types of structural abnormalities include uterine fibroids, endometrial polyps, and adenomyosis, a form of back-bleeding where some blood seeps back into the uterine muscle wall instead of just exiting out the cervix. Structural abnormalities are more common age 35 and beyond. Structural abnormalities are also more common in women who are overweight, even in younger overweight women.
Uterine fibroids are usually non-cancerous tumors that develop in the muscle wall of the uterus. Most women have fibroids but don’t know it because they remain asymptomatic. However, elevated levels of estrogen cause fibroids to grow and multiply. Fibroids that grow rapidly or become very large can contain cancer cells and need to be surgically removed.
Uterine fibroids may cause abnormal bleeding in several ways. Some fibroids may block the uterus from contracting properly, leading to prolonged bleeding. Uterine fibroids can put pressure on the endometrium (the uterus lining), causing heavy bleeding. Uterine fibroids may stimulate the growth of blood vessels, which may cause spotting in between periods.
Adenomyosis is caused when endometrium tissue (cells lining the inside of the uterus) grows into the outer muscular walls of the uterus (the myometrium). This leads to the thickening and enlarging of the uterus, which often causes painful and/or heavy periods. Adenomyosis may cause the uterus to swell and enlarge during a menstrual period.
GYNECOLOGICAL CANCERS
All types of gynecological cancers may cause abnormal uterine or vaginal bleeding. However, it is possible to have a gynecologic cancer that does not bleed. For example, some cancers of the uterus lining do not bleed, and some large fibroids do not bleed.
Unusual vaginal bleeding, heavier bleeding, and bleeding during sex are common symptoms. In some cases, they may be a sign of cervical cancer. The best way to know for sure whether or not your abnormal bleeding is being caused by cervical cancer is to have an evaluation by a gynecologist including an exam of your cervix to check for visible changes. While a pap smear and a check for infection is also important, a physical examination by a gynecologist is extremely important. In some cases, a pap smear may be negative and reassuring but there may be changes on the cervix that represent cancer or pre-cancer.
Uterine cancer symptoms include vaginal bleeding after menopause or between periods. Surgery can cure uterine cancer (including endometrial cancer and uterine sarcoma) if caught before it spreads. Keep track of any bleeding you experience and review the pattern with a gynecologist. There are office tests such as hysteroscopy where a gynecologist can look directly into the uterine lining and get tissue samples to determine if the bleeding represents uterine cancer or pre-cancer.
Vaginal cancer is very rare. Signs and symptoms of vaginal cancer may include post-menopausal bleeding, abnormal bleeding, bleeding between periods or after sex, pelvic pain, lumps in the vagina, and more. Though these symptoms may be caused by something other than vaginal cancer, speak with a doctor for expert advice and analysis.
Although it is possible for ovarian cancer to cause abnormal bleeding and irregular periods, abnormal bleeding is not the most common symptoms of ovarian cancer. The most common symptoms of ovarian cancer are pelvic pain, bloating, abdominal pain, feeling full too soon after eating.
INFECTIONS
Sexually transmitted infections (STIs,) also known as sexually transmitted diseases (STDs,) may cause abnormal uterine or vaginal bleeding. For example, Chlamydia causes inflammation that may lead to bleeding in between periods. Chlamydia can also cause vaginal bleeding after sex. Gonorrhea is another STI that may cause vaginal bleeding in between periods. Often these infections are silent with no pain or discharge or bleeding to signal they are present.
MEDICATIONS
Irregular bleeding is a side effect of several medications. Most of these medications affect hormone levels. These medications are listed under hormonal causes of abnormal bleeding.
HORMONAL MEDICATIONS
Hormones contained in birth control treatments affect bleeding. Birth control pills are often used to control or regulate bleeding in young women, however, there may be abnormal bleeding with the oral contraceptive pill itself, especially while adjusting to it. Birth control pills typically affect bleeding the most during the first 2-3 months. Women with heavy or irregular or prolonged cycles, may return to these types of bleeding patterns when they stop taking oral contraceptive pills.
Before starting hormone therapy in post menopause, it is important to have your gynecologist check that your uterus is normal and there are no pre-cancers or cancers. Women in perimenopause who have irregular menstrual periods and start hormone therapy or replacement also need this baseline check to be certain there are no problems in the uterus lining prior to beginning hormones.
Certain hormonal medications, often used to treat breast cancer, may cause abnormal uterine bleeding. The most well known medication of this type is Tamoxifen. Sold under the brand name Nolvadex, Tamoxifen disrupts hormones by modulating estrogen.
Medications for depression and other mental health disorders may cause abnormal bleeding. Research to understand the relationship between depression and medications to treat it is in the early phases. It is not yet clear what the relationship is between anti-depressants and abnormal bleeding. So far, one study showed that 24.6% of women taking antidepressants experienced menstrual irregularities, with abnormal bleeding being the main type of irregularity. This is compared to the control group, of which only 12.2% of women reported menstrual irregularities. This may be early evidence that women taking anti-depressants could be twice as likely to experience abnormal bleeding compared to women who do not.
Anti-depressants that possibly cause abnormal menstrual bleeding include:
- Selective Serotonin Reuptake Inhibitors (SSRIs) such as Zoloft or Prozac
- Cyclic antidepressants (including Tricyclic and tetracyclic anti-depressants) such as mirtazapine
Antipsychotics such as risperidone and clozapine.
Abnormal bleeding is a well-known side effect in women taking blood thinners. While these medications do not cause bleeding to start, they may make bleeding heavier or last longer than it otherwise would.
Common blood thinners that may cause irregular menstrual bleeding include:
- Aspirin
- Edoxaban
- Warfarin
Corticosteroid medications taken by mouth or given as injections or intravenously, such as cortisone, hydrocortisone, and prednisone are commonly used to treat inflammation, asthma, hay fever, rashes, and more. Long term use of some corticosteroids may interfere with female sex hormones and cause periods to be longer and/or heavier.
Just because a medication is herbal or considered a supplement does not mean the medication does not have side effects. In fact, several popular supplements may cause irregular bleeding by altering hormone levels or affecting the way the blood clots.
Supplements known to cause irregular menstrual bleeding in some women include:
- Ginseng
- Gingko Biloba
- Soy protein
- St. John’s Wort
RETAINED FOREIGN BODIES
Leaving a tampon in for prolonged periods of time can cause infection, abnormal bleeding, and- in severe cases, a life-threatening bacteria illness (Toxic Shock Syndrome).
In some instances, there is adjustment or irregular bleeding when certain types of IUDs are initially inserted. This is most common in the first 3-6 months. IUD’s that have no low hormone release may makes menstrual periods heavier. IUD’s that contain a low dose of slowly released progesterone released locally into the uterus lining typically make menstrual periods shorter and lighter over time, and may even eliminate menstrual periods in some women.
Researchers report a higher likelihood of hormone abnormalities in people that have experienced brain injuries. For women, traumatic brain injuries can cause many menstrual problems including irregular bleeding, amenorrhea, and skipped periods. These irregularities can last as short as one month or go on for many years.
DISEASES
Your thyroid helps regulate hormones associated with your menstrual cycle. The overproduction or underproduction of thyroid hormones may result in skipped, light, or heavy periods.
OTHER MEDICAL CONDITIONS
During a women’s reproductive years, the most common cause of abnormal uterine bleeding is abnormal pregnancy. Light bleeding during the early stages of pregnancy is normal. However, heavy bleeding may indicate a miscarriage or ectopic pregnancy. Other less common causes of pregnancy related bleeding include problems with the placenta such as placenta previa, abruptio placentae, and trophoblastic disease.
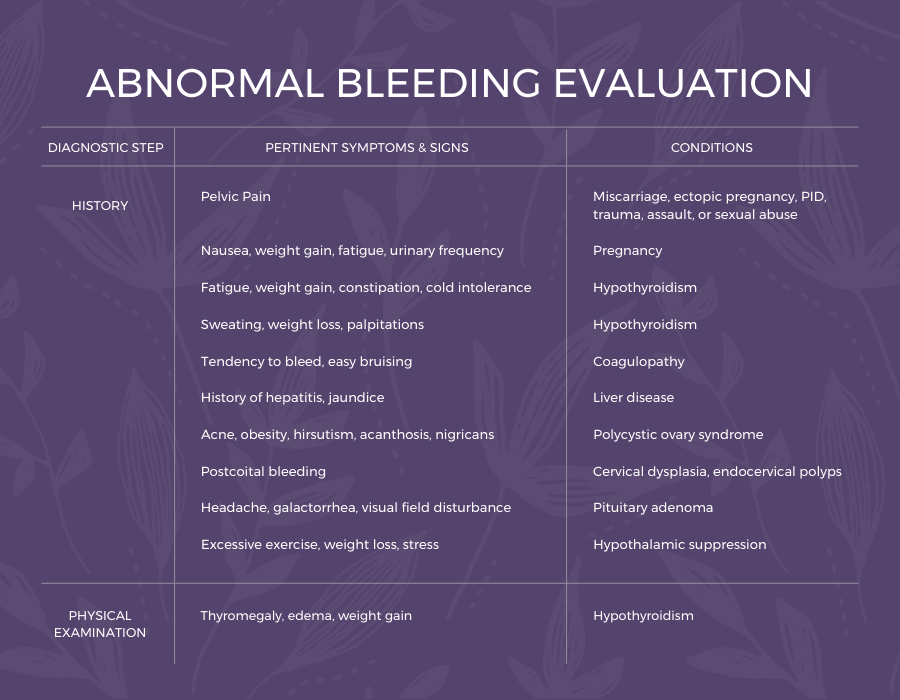
ASSESSMENTS AND DIAGNOSIS of ABNORMAL UTERINE BLEEDING
CLINICAL ASSESSMENT
The first step toward diagnosing the cause of abnormal menstrual bleeding is a clinical assessment from a gynecologist. During this assessment, your doctor will inquire about several things, including:
Your doctor will take your medical history and your family’s medical history. Questions may regard past or present illnesses, past surgeries, history of pregnancy, medication use, and more.
Your doctor will want to screen for any environmental factors, such as stress, that may contribute to menstrual irregularity. The doctor may also ask about any sudden weight loss or weight gain.
Your doctor or gynecologist will ask about any medications you are taking. Many different types of medicine can cause abnormal uterine bleeding. When bleeding is a side effect of a medication, it is known as an iatrogenic cause.
Medications your doctor may inquire about include:
- Hormonal medicines (like hormone replacement therapy or hormonal birth control)
- Anticoagulants (blood thinners)
- Antidepressants
- Corticosteroids
- Herbal Supplements
Presenting your doctor with a record of your menstrual history provides invaluable data during the diagnostic stages. Refer to the “MAINTAINING A MENSTRUATION HISTORY” section to learn more.
PHYSICAL EXAM
After taking your history, your doctor may perform a physical exam. These exams may include:
A pelvic exam allows your doctor to physically examine your pelvic organs to determine if the bleeding is coming from your vagina or vulva instead of your uterus. During the exam, your doctor can also access your cervix, uterus, and ovaries. This allows your doctor to feel for irregularities and identify any painful spots.
A pap smear collects a small sample of cells from your cervix. The sample is tested for abnormal cells to screen out cervical cancer.
DIAGNOSTIC TESTS
Generally, sexually transmitted infections do not cause heavy menstrual periods, but they may commonly cause spotting or bleeding after sex.
Ultrasound using sound waves to image the uterus, cervix uterus lining, muscle wall and ovaries is helpful to learn more about the pelvic structures. Typically, there is no pain or bleeding with an ultrasound test. An ultrasound alone cannot diagnose uterine or cervical cancer but is helpful in learning more about the pelvic structures and pinpointing what other tests are helpful.
A microscopic exam of the uterus lining allows a gynecologist to see the lining tissue and the uterine cavity directly and determine the best place to get a tissue sample. This is the standard for diagnosing cancer and pre-cancer of the uterus lining.
Gynecologist Near Me
If you think you may experience abnormal bleeding, don’t ignore it. Schedule a consultation with Dr. Julia Edelman. She is renowned in the field of women’s health and can answer all your questions, diagnose your symptoms or problems, and offer non-invasive solutions using groundbreaking technology and the latest techniques in treating abnormal bleeding.
Reach out to Dr. Edelman at Women’s Health and Gynecology of New England, PC today by calling 508 947-0800 to schedule your consultation. You can also contact Dr. Edelman online by filling out the form below.
Schedule a
Menstrual Bleeding Treatment Consultation
Please call 508-947-0800 or fill out the form below
By submitting this form you agree to be contacted via phone/email
SOURCES
Menopause Matters. Julia Edelman, MD, FACOG, NCMP LINK.
Murke, M. P., Gajbhiye, S. M., Amritwar, A. U., & Gautam, S. R. (2011). Study of menstrual irregularities in patients receiving antipsychotic medications. Indian journal of psychiatry, 53(1), 79–80. https://doi.org/10.4103/0019-5545.75550. LINK.
Uguz, F., Sahingoz, M., Kose, S. A., Ozbebit, O., Sengul, C., Selvi, Y., Sengul, C. B., Ayhan, M. G., Dagistanli, A., & Askin, R. (2012). Antidepressants and menstruation disorders in women: a cross-sectional study in three centers. General hospital psychiatry, 34(5), 529–533. https://doi.org/10.1016/j.genhosppsych.2012.03.014. LINK.
DISCLAIMER
*You agree to be contacted by Women’s Health and Gynecology of New England, PC regarding marketing messages by text, phone, or email, by submitting this form. We respect your private information and commit to protecting it. At any time you are able to unsubscribe from these messages. For more information regarding our Privacy Policy, please review here.
Schedule a
Menstrual Bleeding Treatment Consultation
Please call 508-947-0800 or fill out the form below
By submitting this form you agree to be contacted via phone/email